Electronic Health Records (EHRs) use diverse data entry models to support various clinical use cases. Each model has specific terminology and information structure requirements. To ensure the captured information is interoperable and meaningful beyond its initial use, it is essential to design a comprehensive context representation model.
The table below outlines common approaches to capturing clinical data and highlights the varying methods used to represent contextual information.
Table 2.2-1: Clinical data entry scenarios and context representation challenges
| Record Entry Type | Record Entry Examples1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
Free text entry | Admission Note Acute
161972006
|
central chest pain (finding)|
. Note after investigation Diagnosis of myocardial infarction. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
Structured form with headed sections |
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||
Structured form with headed sections and prompts for specific data items |
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||
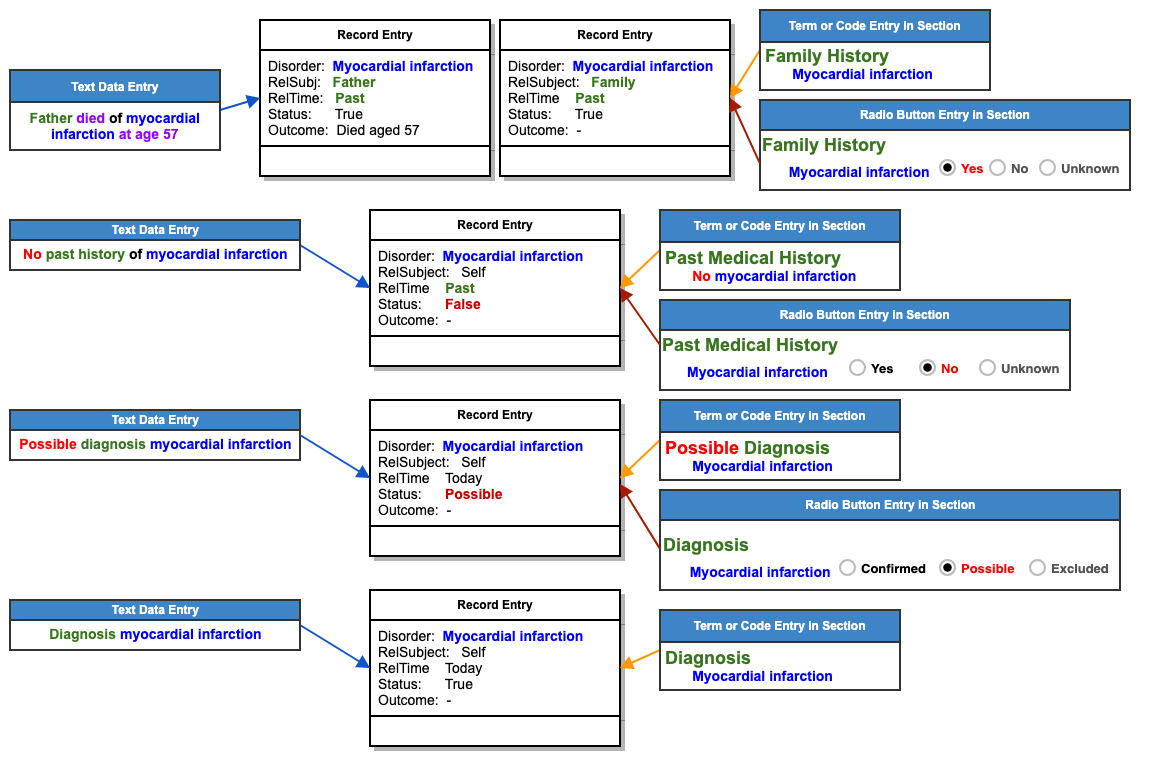
An EHR may be structured in ways that enable data collection and display in structures that emulate the preexisting paper-based record structures. However, there is a significant difference between the structure of a paper record entry and the structure of an electronic record. The structure in which a paper record is stored and displayed is determined by the way the entry was written. In contrast, data entered in an electronic health record (EHR) through different user interfaces may be stored in a common logical data structure. Provided that the logical structure contains the necessary data, the record can be displayed, reported, and analyzed in different ways. This means that different data entry techniques may be appropriate in different situations. For example, in some situations, a fixed checklist of key questions about broadly relevant items of past medical history and family history may be appropriate. In other situations, a more complete and detailed approach appropriate to a specific diagnosis may be preferable. In a paper-based record, these different approaches lead to records with different structures containing similar information. However, as illustrated in Figure 2.2-1, a well-designed electronic health record system can store similar information in a common form even if it is collected through different user interfaces.
Accurate interpretation of clinical data entered in different ways requires the EHR system to capture, and consistently interpret, information associated with the context in which data is entered. For example, to clearly distinguish between a confirmed diagnosis, possible diagnosis, past medical history, or family history of a disorder. Techniques that can be used to meet this requirement are discussed in the next section 4.2 Health Record Context.
Figure 2.2-1: Example of Mapping from Different User Interface Examples to a Common Data Structure
Footnotes
This column contains abbreviated examples of record entries that illustrate points made in this section. More extensive examples of records are provided in Appendix C. Health Record Structure Examples.
The concept representing Gaviscon is in the UK National SNOMED CT Extension (see https://termbrowser.nhs.uk/?perspective=full&conceptId1=3402011000001103).
Feedback
Overview
Content Tools
Apps