Date: 2018-01-26
1600 UTC
Zoom Meeting Details
SNOMED Int'l Editorial Advisory group
SNOMED International - Editorial advisory group conference call
UTC
Please join my meeting from your computer, tablet or smartphone
https://snomed.zoom.us/j/807454545
Attendees
Chair:
AG Members
Meeting Files
Objectives
- Obtain consensus on agenda items
Discussion items
| Item | Description | Owner | Notes | Discussion | Action |
|---|---|---|---|---|---|
| 1 | Call to order and role call | JCA |
| ||
| 2 | Conflicts of interest Approval of minutes from Bratislava | JCA | No conflicts reported | No conflict of interest reported. |
|
| 3 | ECE Update | BGO |
|
See Events, Conditions, Episodes Project Group meeting agenda 2-12-2018 | |
| 4 | Drug Model Update | TMO | Toni Morrison to provide an update on the status of the drug project | Document with schedule and content changes attached to minutes. There will be changes to the MRCM including GCIs and role chaining that facilitate the modeling of drug products. This is needed to support the flattening of the substance hierarchy but still allow hierarchical representation in other hierarchies that use these substances as defining relationships. These changes also allow for multiple sufficient definitions. | |
| 5 | Observables Model Update | DKA | Not available | ||
6 | Revision of editorial guidance for PATHOLOGICAL PROCES concerning "Inflammation (qualifier value) | JCA | Current editorial guidance on the use of the Pathological Process Value = 257552002 Inflammation (qualifier value) The current editorial guidance on the use of this process value eventually resulted in the need to distinguish between process and structure in the Morphologic abnormality hierarchy. E.g. 23583003 |Inflammation (morphologic abnormality)| vs. 409774005 |Inflammatory morphology (morphologic abnormality)|. There is a tracker item: IHTSDO-558 Initial draft Fast track document : https://docs.google.com/document/d/1r1x9hoW4S4s5gO0Ce9pHth6ofkI6UJhfzfEUtS1l-8U/edit Questions:
This notion is critical to the continued improvement of content in SNOMED CT; however, it adds substantial complexity and will require clear and possibly extensive guidance to ensure consistent application. Templates may be the most efficient way to guarantee compliance. | Examples of where additional pathological process values include the hypersensitivity condition subhierarchy and the use of "Pathological development process" for congenital malformations. Expanded range of PATHOLOGICAL PROCESS may allow for a substantial number of currently primitive concepts to become fully defined. Many current morphology concepts conflate process and structure. Many of these may have originated from early versions of ICD-O. There are not many "process" concepts in SNOMED, but these may be needed in the future. One question is whether we should investigate the defining of the structures based on the processes that lead to the structure. Another suggestion is that it may not be necessary to do a full reconstruction of pathological processes, but do a focused effort on areas that have been problematic due to the lack of a defining process. In other words, add them as needed to meet a particular modeling problem. There are a number of "idiopathic" diseases, which really indicates an "unknown" process. It is not a negation of the other process, it is just an indication of a lack of knowledge of the specifics of the process. This would indicate a positive assertion of being unknown. Any changes to pathological process may have broad ranging impacts on the terminology. Does it need external review and approval? Input from the group is that there should not really be substantial taxonomic changes, only clarification and improvement. |
|
| 7 | Disorder without disorder | JCA | Common pattern in classifications such as ICD. Currently all are primitive in SNOMED CT. One potential modeling pattern proposed is the use of the Situation model with one "known present" relationship group and one "known absent" relationship group. The problem with specific negation is that it is silent about other clinical aspects that may be of significance. What is the purpose of calling out one specific clinical manifestation? Comments solicited from, CMAG: Use of concepts representing the presence of a disorder without a second disorder | Current modeling of disorder with disorder is in Clinical findings, whereas these would need to be located in the Situation hierarchy. Opinion from CMAG is that this is primarily a construct used to map to ICD, but not used much in clinical practice. Jeff PiersonSees these as primarily classification concepts. Would be useful to see how often these are used for clinical recording. Jeremy Rogers agreed with this, not very useful clinically except in very specific cases. Procedure without procedure is a more common pattern used by surgeons. Generally thought that these were useful only for ICD mapping. Guillermo Reynoso suggested that this should in general be handled at the information model level. Q: What should we do with the current content that is all primitive? The best way to express this is to override the default context by an explicit wrapper in the information model. It would be important to try to remove this implicit context in future redesigns of SNOMED CT. |
|
| 8 | Lexical inconsistencies | JCA | We received a comment from a dutch lexographer: Dear fellow terminologist(s), | Guillermo Reynoso mentioned that while this is primarily an English language issue, it does affect translations and the consistent use of the hyphen (not the dash or the em-dash as they require extended character set) is preferable. Would need to develop editorial rules on how to apply these consistently to the terminology, including guidance on no spaces before and/or after the hyphen. Capitalization issue: This is a legacy issue that originated with the initial SNOMED content from the 1960s. Many translations do not use initial capitalization. Recent changes to case significance may make this a difficult issue to resolve. This should have been corrected prior to the history tracking. Suggested that we remove the current requirement to have an initial capital for new concepts moving forward and living with the "sins of the past". Fixing this would require changes to over 1 million descriptions and this would be too much churn for little value. Rationale is that this change would make SNOMED consistent with ISO 704. |
|
| 9 | Specimen from subjects other than the patient | JCA | Currently we have many concepts in the specimen hierarchy that include “from patient”as well as those that do not include it as an ancestor. Since the subject of record is the default for specimens, we would like to retire these apparent duplicates, but then we run into the problem of specimens derived from other sources such as donors or normal control patients. They cannot be subtypes if the intended meaning is “subject of record”..or can they, since the context is implied? How do we structure the specimen hierarchy to account for this? What are the analytical implications of having different sources for specimens as subtypes of one another? Tracker: IHTSDO-1001 - Getting issue details... STATUS | No testing of options for this item has been performed since the last meeting. Issues still remaining:
| |
| 10 | What is an "infected prosthesis" | JCA | Update: Proposed model (Infected Prosthesis) was tested and reviewed by the ECE. Construction has been performed and editorial guidance will be updated as necessary |
| |
| 11 | “Acquired” disorders testing | JCA |
Update: A grouper "period of life" term encompassing all stages of life (Postnatal (qualifier value)) after birth was created. Over 100 concepts with the string "Acquired" were reviewed and fully defined using the OCCURRENCE attribute. There were no adverse impacts from this initial test. One conditional issue relates to the ability to define terms with the string "juvenile". The definition of juvenile differs in age ranges from jurisdiction to jurisdiction. Likewise the definitions of age ranges for "childhood" and "adolescent". There is an inactive concept 282035009 - Juvenile (qualifier value) that was once a subtype of "Period of life", but was inactivated as duplicate to 59223006 - Juvenile (finding). The process to progress this needs to be determined. | 2017-11-03: A related tracker exists: PCP-71. The work related to this item will be linked to that tracker. Issue identified during testing was the perceived need for the concept "juvenile", which is an inactive concept. Concern about how many concepts will be affected. Will all concepts that are known to be acquired have this attribute added? No, only concepts that need a differentiation between a congenital and acquired form. It may not even be necessary to have as many periods of life as we currently have. While the results of testing are encouraging, it is better to have another attribute that can be role grouped than to create a primitive parent to be used as an IS A due to the advantages that come out of classification. The current testing has resulted in very few changes to the existing taxonomy, but makes the content more maintainable. Juvenile concepts may still be needed, but can be put off for later consideration (can be modeled with postnatal until then). |
|
| 12 | Update of EAG Workplan | JCA | Review and revision of current workplan | Continued to next call due to lack of time. |
|
| 13 | Future meetings | JCA | TBD |
|
5 Comments
Penni Hernandez
Could there be a calendar created for this group's meetings so it could be added to a google calendar?
Jim Case
Sure, if I knew how
Jeremy Rogers
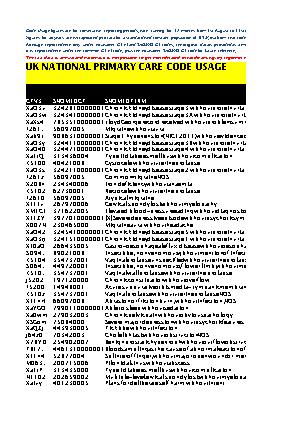
Data on code usage within UK Primary Care in respect of 'disorder without disorder' type codes was (apparently) already passed by me via Elaine Wooler to the related CMAG discussion last December
Jim Case
Jeremy Rogers Can we attach those data to the minutes here?
Jeremy Rogers
Try this: