Date and time
2020-10-19 20.00 UTC
Zoom Details
Apologies
Objectives
Discuss and make progress on these issues:
- Review of previous issues
- Observables and Evaluation procedures
Discussion items
See below.
| Item | Description | Owner | Notes | Action | |
|---|---|---|---|---|---|
| 1 | Welcome & apologies | Remember recording! | |||
| 2 | Conflicts of interest | ||||
| 3 | Minutes from previous meeting | Daniel Karlsson | |||
| 4 | Mental Function observables | Piper Allyn Ranallo is doing a mental health clean up based on Mental & Behavioral CRG work - she has submitted some requests for editing and applying the observable entity model to existing content: 285231000 |Mental function (observable entity)|, 8373002 |Nervous system function (observable entity)|, 4065008 |Affect, function (observable entity)|311465003 |Cognitive functions (observable entity)|. Need advice on applying the model to these function observables. Hello Daniel and Suzanne I have now received a reply from Piper to Daniel's questions:
2020-04-20: Daniel Karlsson participated on MBHCRG call 2020-04-08. A central issue is two aspects of mental function observables, e.g. Folstein MMT asks about the current date, but the function studied is the ability to orient in time. The raw value is a date, but the clinical value is about function. Observables preferably should allow representation of both aspects. 2020-06-15: Need for clarification of what "function" means in function observables. Other MBHCRG issues. 2020-07-20: James R. Campbell presented a hierarchy of "neuropsychological" processes. We agreed to contact the MBHCRG through the liaison Paul Amos to start getting agreement on such a hierarchy, likely to be a central piece in definition of MBH observables. 2020-08-17: With participation from the Mental and Behavioural Health CRG, James R. Campbell presented the neuropsychological processes. Piper Allyn Ranallo asked the group how to progress the work that MBHCRG needs to do to better define both Clinical findings and Observables in the MBH space. One concern is the demarcation of process observables on the one hand and process qualifier values on the other. Due to a large legacy of existing not always well-represented Observables, trying to make sense of the current MBH observables is likely not a worthwhile effort. It was suggested to focus on use cases that need to be represented in SNOMED and then see what concepts are needed both to define Observables and Clinical findings and to allow those respective hierarchies to reflect the intended meaning. | Daniel Karlsson Send email to Paul Amos and Piper Allyn Ranallo (CC James R. Campbell) to initiate discussion about Nebraska mental process hierarchy | ||
| 5 | Dentistry observables | At a Dentistry CRG meeting 2020-08-05 it was requested that the Observables PG discussed observables for count of teeth with caries of various types (active and arrested particularly), likely children of 251319000 | Decayed tooth count (observable entity) |. See Dentistry page. Discussion will be held next call (2020-09-21)! 2020-09-21: Slides on use of component for defining count of carious teeth: https://docs.google.com/presentation/d/10t0zEBwtR5-RpUN4nAwS281HZdsavecZ5aXS4RufnfM/edit?usp=sharing Definitions both in the Observables model and Evaluation procedure model needs to aligned and updated. |
| ||
| 6 | Target observables | The issue of representation of target observables has been raised again in a Jira ticket. The question the group needs to answer is whether targets and observables need to be seperated or to be kept apart. In practice, is there a requirement to query for both observables and "settings" alternatively is there a risk in having targets and observations mixed up? One solution would be to (minimally) add a primitive parent "setting observable" (or just "setting") to all targets, settings, parameters, etc. in the current observables hierarchy. 2020-09-21: Suzanne Santamaria shared with the nutrition group, will share with Jim Case 2020-10-19: DIscussion about flavours of word "target", "goal" etc. Suggestion to add a single "target observable" primitive for now and work with other types of "settable" observables as the need arises. |
| ||
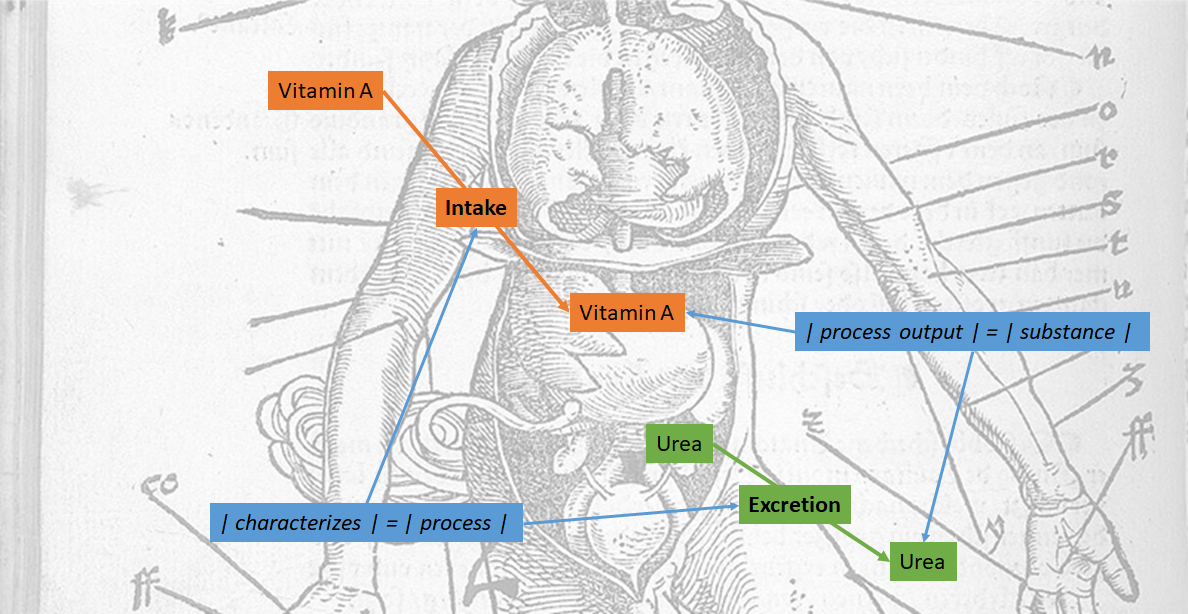
| 7 | Process observable attributes | X | The use of attribute | process output | for intake observables is at least mildly confusing. Is there a need for updated guidance or clarification?
2020-02-24: Guidance needs clarification. This particular attribute is difficult to explain and often needs re-explaining(!). Alternatives | process target |? 2020-03-16: Check existing use of the attribute in the SNOMED release as well as in the LOINC linking results. 2020-04-20: Deadline for MRCM changes has passed, so more time is available for analysis. All LOINC expressions with | process output | are also | characterizes | = | excretory process |. The other | process output | Observables are <<364075005 | Heart rate (observable entity) | and <<86290005 | Respiratory rate (observable entity) |. 2020-05-18: Use case from histopathology: representation of invasion.
2020-06-15: Update of range of | process output | to include Products. 2020-07-20: Slides updated. Use cases presented compared to other ontology work, primarily the Relations Ontology of BFO. The use case from CSRPG (specifying the anatomic structure into which a neoplasm has proliferated) seems not to be supported by any single attribute. Recommendation is to use | process output | until this issue is resolved and a batch update can be made. 2020-09-21: (More than) Time to decide on new attributes: https://docs.google.com/presentation/d/1zdM5Ld4H74GCmelaH0K1a5DlnK7ETSQpVFezgpdUEDY/edit?usp=sharing 2020-10-19: Editorial guide pages needs updating. |
| |
| 8 | Tumor observables | X | Around 200 observable entity concepts include "tumor" in the FSN and around 50 observable entity concepts include "neoplasm" or "neoplasia" in the FSN. "Tumor" is considered ambiguous by SI (described in the specific disorder modeling section of the SNOMED CT Editorial Guide here: https://confluence.ihtsdotools.org/display/DOCEG/Specific+Disorder+Modeling). However, "tumor" is used in this morphologic abnormality modeling section of the Ed guide: https://confluence.ihtsdotools.org/display/DOCEG/Morphologic+Abnormality+Modeling. Tumor observable entity content has been considered for use in the Cancer Synoptic Reporting Project work; 395531003 |Tumor observable (observable entity)| is one of the high level concepts that currently subsumes much of their content being developed in an extension which will be a candidate for promotion to the international release in the future. Scott Campbell brought up the issue of what to do with the tumor observable content as he tends to think "tumor" is ambiguous. CAP uses "tumor" in their worksheets but it specifically means "primary malignant neoplasm." Scott will try to obtain some usage data on the current SNOMED CT tumor observable concepts. An initial conversation with one CAP representative revealed that he did not see much of an issue with using "tumor" in the FSN of the content because tumor and neoplasm are equivalent in his mind. Some initial options to consider:
Consider providing early release notice or BN if any option involving inactivation of content is chosen. 2020-07-20: JIRA ticket: OBSERVABLE-4 - Getting issue details... STATUS Jim Case have given go ahead to change FSN of Tumor observable to Neoplasm observable and to author a new concept Proliferative mass observable, a super concept of Neoplasm observable. The definition of this new observable might need a GCI to represent that the neoplasm can have different roles in different observables, e.g. | inheres in | or | component |. |
| |
| 9 | Observables and Evaluation procedures | Since Observables were introduced into SNOMED CT the demarcation between Observables and Evaluation procedures has been a potential source of variability of SNOMED CT use. In order to progress this issue the group need to agree on what knowledge is needed to inform any future decision. 2019-11-18: <<404684003 |Clinical finding (finding)| : 363714003 |Interprets (attribute)| = << 386053000 |Evaluation procedure| ==> 7148 concepts ...but also 1350 hits for <<386053000 | Evaluation procedure (procedure) |: [2..*] { 260686004 |Method (attribute)| = <<129265001 |Evaluation - action (qualifier value)| } 3 hits for <<386053000 | Evaluation procedure (procedure) |: [2..*] { 260686004 |Method (attribute)| = <<129266000 |Measurement - action (qualifier value)| } 611 hits for <<386053000 | Evaluation procedure (procedure) |: [2..*] { 246093002 |Component (attribute)| = * } 2019-12-16: Some more exploration of existing Evaluation procedure content: (<<386053000 |Evaluation procedure (procedure)| : [2..*] { * = * }) MINUS <<363679005 |Imaging (procedure)| 10 000-ish Evaluation procedures have 2 or more role groups... <<386053000 |Evaluation procedure (procedure)| : [2..*] { 246093002 |Component| = * } 611 have 2 or more Components, indicating that it could be a panel. However, many examples are just strangely modeled and likely not intended to be panels. Thus, it's not straight forward to identify panel-like procedures among the Evaluation procedure. Sometimes, e.g. 442553005 | Measurement of chloride in peritoneal fluid specimen (procedure) |, additional Components are inherited from ancestors. (<<386053000 |Evaluation procedure (procedure)| : [2..*] { 246093002 |Component| = * }) MINUS <<122869004 |Measurement procedure| Even non Measurement procedures have multiple Components... <<386053000 |Evaluation procedure (procedure)| : [3..*] { 246093002 |Component| = * } A few have 3 or more components, many of which are in fact panels, but again likely not all of them. E.g. see <67899004 | Complement component, classic pathway (substance) |. Briefing note should include:
2020-01-28: The issue of panel concepts (sets of distinct Observable entities) was discussed. The current Observables model, by design, does not allow representation of panels. Many examples of panels are not well-defined, e.g. a Complete Blood Count may contain different observables in different laboratories. The benefit of adding content on the international level is likely limited. However, SNOMED CT should provide the means to represent such panels when there is agreement on meaning on a national, regional or local level. Several Evaluation procedure concepts contain multiple groups, but all are not correctly modelled. 2020-02-24: Aim to get feedback from members about usage of Evaluation procedures. Further aim to identify candidates for Procedure-to-Observables transfer, i.e. Procedure concepts which represent observations which has a single, distinct result/value. Some gaps exist in creating observables corresponding to those procedures, most notably techniques are missing. 2020-03-16: The topic has been lifted in the Modeling Advisory Group. Panels (aka observables without values): Examples of types of panels are groupers for lists, screening and function tests. Naming today is insufficient to distinguish from e.g. totals (e.g. amino acid panel vs. total amino acid etc.). Definition and naming of panels (observables OR evaluation procedures). 2020-04-20: EAG + MAG meeting to be planned. Preparation meeting held (slides). | |||
| 10 | Next meeting | Next meeting is 2020-11-16 20.00UTC | |||
| 11 | AOB |


{kind=link}
{kind=link}
Previous Meetings
| Title | Creator | Modified | |
|---|---|---|---|
| E2O meeting 20220825 | Daniel Karlsson | 2022-Aug-25 | |
| 2022-05-23 - OBSERVABLE Meeting | Daniel Karlsson | 2022-May-24 | |
| E2O meeting 20220504 | Daniel Karlsson | 2022-May-05 | |
| 2022-04-25 - OBSERVABLE Meeting | Daniel Karlsson | 2022-Apr-26 | |
| 2022-04-06 - OBSERVABLE Face-to-face Meeting | Daniel Karlsson | 2022-Apr-25 | |
| 2022-03-21 - OBSERVABLE Meeting | Daniel Karlsson | 2022-Mar-31 | |
| E2O 23rd meeting 20220223 | Daniel Karlsson | 2022-Feb-23 | |
| 2022-02-21 - OBSERVABLE Meeting | Daniel Karlsson | 2022-Feb-22 | |
| E2O 22st meeting 20220202 | Daniel Karlsson | 2022-Feb-02 | |
| 2022-01-24 - OBSERVABLE Meeting | Daniel Karlsson | 2022-Jan-24 | |
| 2021-12-20 - OBSERVABLE Meeting | Daniel Karlsson | 2021-Dec-20 | |
| 2021-11-15 - OBSERVABLE Meeting | Daniel Karlsson | 2021-Dec-16 |
More Zoom details
Topic: Observables meeting
Time: this is a recurring meeting Meet anytime
Join from PC, Mac, Linux, iOS or Android:
https://snomed.zoom.us/j/992630241
Or Telephone:
Dial:
+46 (0) 8 4468 2488 (SE Toll)
+61 (0) 2 8015 2088 (AU Toll)
+32 (0) 2 588 4188 (BE Toll)
+1 647 558 0588 (CA Toll)
+56 41 256 0288 (CL Toll)
+420 2 2888 2388 (CZ Toll)
+45 89 88 37 88 (DK Toll)
+372 880 1188 (EE Toll)
+852 5808 6088 (HK Toll)
+353 (0) 1 691 7488 (IE Toll)
+972 (0) 3 978 6688 (IL Toll)
+370 5214 1488 (LT Toll)
+60 3 9212 1727 (MY Toll)
+356 2778 1288 (MT Toll)
+31 (0) 20 241 0288 (NL Toll)
+64 (0) 9 801 1188 (NZ Toll)
+64 (0) 4 831 8959 (NZ Toll)
+47 2396 0588 (NO Toll)
+48 22 307 3488 (PL Toll)
+351 308 804 188 (PT Toll)
+65 3158 7288 (SG Toll)
+421 233 056 888 (SK Toll)
+386 1888 8788 (SI Toll)
+34 91 198 0188 (ES Toll)
+41 (0) 31 528 0988 (CH Toll)
+44 (0) 20 3695 0088 (GB Toll)
+1 408 638 0968 (US Toll)
+1 646 876 9923 (US Toll)
+1 669 900 6833 (US Toll)
Meeting ID: 992 630 241
International numbers available: https://snomed.zoom.us/zoomconference?m=AQWV2VqAIGYWMcMapl9CoYjsaj1TVS7K